
Paulo Eduardo Ocke Reis
Department of Specialized and General Surgery, Fluminense Federal University, Rio de Janeiro, Brazil
Corresponding author:
Paulo Eduardo Ocke Reis
vascular@pauloocke.com.br
Department of Specialized and General Surgery, Fluminense Federal University, Rio de Janeiro, Brazil.
Tel: +55 21 2629-5000
Citation: Reis PEO. Ovation: The Sealing O-Ring–New Co
[blank h=”15″]
[/blank]
In 1991, Dr. Juan Parodi described, for the first time, the exclusion of an Abdominal Aortic Aneurism (AAA) from circulation using an endovascular approach. He showed that a perfect seal zone between the endograft and the aortic wall was necessary to completely exclude the AAA [1]. Today, Endovascular Aneurysm Repair (EVAR) has replaced open surgical repair as the most common method of treatment for AAA. Controlled trials, including the EVAR Trial 1, one and two year results and the DREAM trial 30 day results, have shown early benefits of EVAR versus open repair in the treatment of AAA, however, the total mortality benefit was lost after two years [2].
Authors agree that complex proximal neck anatomy represents one of the most common contraindications for commercially available devices, complications such as type I endoleaks, kinking, and migration could be related with aortic sac rupture and death [2-6]. Additionally, enlargement of the infrarenal aortic neck has been reported after EVAR interventions [7]. Though EVAR can be used in patients with short aortic necks, it is associated with type I endoleaks as found in Aburahma et al. [8].
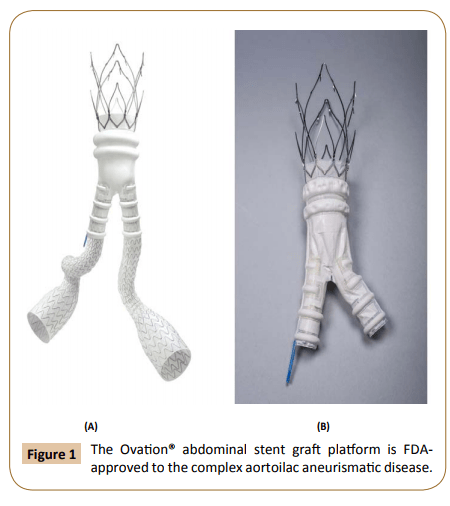
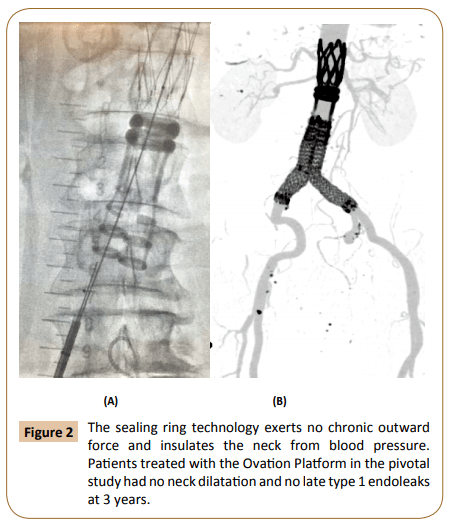
The Ovation® Abdominal Stent Graft System (Ovation System) (Endologix Inc., Santa Rosa, Calif) (Figure 1) is a recently approved trimodular bifurcated device that has a new concept of sealing, using polymer based technology to create a patient specific sealing O-Ring. The Ovation System is comprised of a main body and two limbs which are delivered via a flexible hydrophilic 13F–14F OD catheter. The aortic body consists of a low permeability Polytetrafluoroethylene (PTFE) graft, and suprarenal nitinol stent with integral anchors; and the iliac limbs are made of nitinol stents encapsulated in PTFE. Once in the appropriate location the Ovation System is deployed in stages. First the graft is fixated in the intended location by deploying the suprarenal anchors and then a patient specific seal is achieved in situ by introducing a low viscosity, radiopaque fill polymer through a network of inflatable channels and sealing rings that cures to the native anatomy of the aorta (Figure 2) [9,10]. The kink-resistant iliac limbs are then deployed on both the ipsilateral and contralateral side to complete the deployment. The Ovation System improves the viability and efficient of EVAR by its ability to treat a wide range of anatomies including difficult anatomies for traditional EVAR [9-11]. Women with AAA, who typically have smaller diameter access vessels, more calcified tortuous iliac vessels, and short aortic necks, may be particularly well suited for the Ovation Systems low profile delivery system that can help “navigate” small diameters access vessels and complex anatomy [9]. A sub-analysis of the Ovation Multicenter Post Market Registry demonstrated that through three year women derived similar benefit to men with EVAR intervention using the Ovation System [9].
There is strong clinical evidence to support the long term durability of the Ovation System’s polymer based sealing O-Ring. For example, the results of De Donato et al. paper on the multicenter registry of patients treated with the Ovation endograft, showed that at three years, that there was no aneurysm-related death, rupture, stent–graft migration, or neck enlargement [12].
Furthermore, the effectiveness of the Ovation System was consistent for patients with short neck lengths defined as <7mm compared to patients with longer aortic necks of ≥7 mm long both groups showing continuous wall apposition with a circumferential non-expansive seal independent of aortic neck length. These results showed that the use of the Ovation System is not restricted by the conventional measurement of aortic neck length, affirming the recent Food and Drug Administrationapproved changes to the device-specific instructions for use to require an aortic neck inner wall diameter between 16 and 30 mm at 13 mm below the inferior renal artery instead of the traditional neck length requirement [12]..
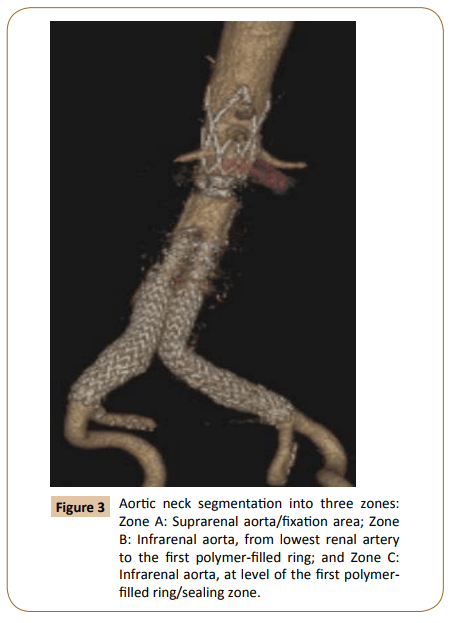
The Ovation System’s sealing O-Ring-new concept is characterized by non-expansive circumferential apposition of polymer-filled rings to aortic wall creating no chronic out-ward force at the infrarenal aortic level. The mechanism for achieving seal is completely different from that obtained by self-expanding stent grafts, with no morphologic changes to isolate the aortic wall neck from blood pressure, thus preventing aortic constantly changing over time (Figure 3) [13].
Additional evidence of the clinical utility of the Ovation Systems O-Ring was shown by Mehta et al. presentation of the 5 year results of the Global Pivotal Trial Data during the, 2016, Veith Symposium [14]. The Ovation Pivotal Trial included a total of 161 patients, enrolled in Chile, Germany and USA from November 2009 to December 2011. Through five years, the key highlights from the data included [14]:
• Broad patient applicability, with 40% of the patients treated outside the labeled indications of other Endovascular Aortic Repair (EVAR) devices.
• Stable aortic neck diameters with an average expansion of 0.1%, compared to 25% as reported with other EVAR devices. 97.5% Freedom from secondary interventions related to type 1 endoleak.
• No migration or conversions.
Dr. Mehta commented, “The five-year data from the Ovation Pivotal Trial confirms the long-term safety and durability of the Ovation system. The study included the broadest range of AAA.” We are optimistic that the Ovation endograft is now a viable and safe option for treating patients with challenging aortic anatomies including short necks, as well as a solution to reduce the incidence of complications such as type I endoleaks, kinking, and migration which are related to aortic sac rupture and death.
[blank h=”15″]
[/blank]
References
1 Parodi JC, Palmaz J, Barone H (1991) Transfemoral intraluminal graft implantation for abdominal aortic aneurysm. Ann Vasc Surg 5: 491-499.
2 Patel R, Sweeting MJ, Powell JT, Greenhalgh RM (2016) EVAR trial investigators. Endovascular versus open repair of abdominal aortic aneurysm in 15-years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomized controlled trial. Lancet 388: 2366-2374.
3 Peterson BG, Matsumura JS, Brewster DC, Makaroun MS (2007) Excluder bifurcated endoprosthesis investigators: five-year report of a multi-center controlled clinical trial of open versus endovascular treatment of abdominal aortic aneurysms. J Vasc Surg 45: 885-890.
4 Wang GJ, Carpenter JP (2008) The Powerlink system for endovascular abdominal aortic aneurysm repair: six-year results. J Vasc Surg 48: 535-545.
5 Stermberg WC, Greenberg RK, Chuter TA, Tonessen BH (2008) Zenith investigators. Redefining postoperative surveillance after endovascular aneurysm repair: recommendations based on 5-year follow-up in the US Zenith multicenter trial. J Vasc Surg 48: 278-285.
6 Kitagawa A, Greenberg RK, Eagleton MJ, Mastracci TM (2013) Zenith p-branch standard fenestrated endovascular graft for juxtarenal abdominal aortic aneurysms. J Vasc Surg 58: 291-300.
7 Diehm N, Dick F, Katzen BT, Schmidli J, Kalka C, et al. (2008) Aorticneck dilatation after endovascular abdominal aortic aneurysm repair: a word of caution. J Vasc Surg 47: 886-892.
8 AbuRahma AF, Campbell J, Stone PA, Nanjundappa A, Jain A, et al. (2009) The correlation of aortic neck length to early and late outcomes in endovascular aneurysm repair patients. J Vasc Surg 50: 738-748.
9 Storck M, Nolte T, Tenholt M, Maene L, Maleux G, et al. (2016) Women and men derive comparable benefits with an ultra-lowprofile endograft: 1-year results of the European OVATION registry. J Cardiovas Surg.
10 Mehta M, Valdes FE, Nolte T, Mishkel GJ, Jordan WD, et al. (2014) One-year outcomes from an international study of the Ovation Abdominal Stent Graft System for endovascular aneurysm repair. J
Vasc Surg 59: 65-73.
11 Reis PEO (2016) Endovascular treatment of infrarenal aortic aneurism with ovation abdominal stent graft system. J Vasc Endovasc Surg 1: 4.
12 De Donato G, Bresadola L, Castelli P, Chiesa R, Mangialardi N, et al. (2017) On behalf of the Ovation Italian Study (TOIS) Collaborators*. Midterm results of proximal aneurysm sealing with the ovation stent-graft according to on-vs off-label use. J Endovas Ther pp: 1-7.
13 De Donato G, Bresadola L, Castelli P, Chiesa R, Mangialardi N, et al. (2015) Aortic neck evolution after endovascular repair with Ovation stent graft. J Vasc Surg pp: 1-8.
14 https://endologix.com/wp-content/uploads/2016/11/elgx-ovation-5-year-data_final-11-15-2016.pdf
[/column]